
Special Surgical Procedures II
LESSON 3: Procedures in Genitourinary Surgery
Section Iv: operations on the bladder and prostate
3-28
3-28. SUPRAPUBIC PROSTATECTOMY WITH CYSTOSTOMY
a. General. This procedure involves enucleation of the prostatic adenomas or hypertrophied masses via a suprapubic approach. It is required because as the male ages, the prostate gland enlarges and gradually obstructs the urethra, giving rise to symptoms of urinary obstruction. The enlargement may be benign or malignant. In benign hypertrophy, only the periurethral portion of the gland is removed. When malignancy is involved, however, total or radical prostatectomy is done. This may involve excision of the entire gland and its capsule, together with associated structures, a portion of the trigone of the bladder, and the seminal vesicles.
b. Patient Preparation. The patient is placed in the supine or modified Trendelenburg position, with the legs apart and the weight of the torso supported by shoulder braces. An O'Connor drape may be fanfolded at the pubis, with the penis exposed through the fenestration and the finger cot in the rectum. A towel folded lengthwise is placed over the fanfolded drape at the pubic level, and a fenestrated disposable drape is used at the site of the suprapubic incision.
c. Operative Procedure.
(1) The bladder is distended via catheter irrigation, as for cystotomy. Vasectomy is frequently done as a preliminary procedure to prevent postoperative epididymitis.
(2) The bladder is approached through the routine cystotomy incision, and the top of the bladder is dissected free, using long thumb forceps and Metzenbaum scissors.
(3) The wall of the bladder is grasped on each side of the midline with Allis forceps. Two traction sutures of chromic gut number 0 on Ferguson number 12 needles may be placed through the wall of the bladder at this point and retained on straight hemostats.
(4) The muscle layers of the bladder are spread by blunt dissection with a hemostat until the mucosa is exposed. Allis forceps are placed on either side, and the bladder is incised, using a scalpel with a number 10 blade. The opening is extended with scissors. Bladder retractors--either long-bladed loops or self-retaining type--are placed, and the bladder is explored.
(5) The surgeon places the forefinger of one hand into the rectum via the finger cot in the O'Connor drape and pushes the prostate gland forward. With the forefinger of the operating hand, the lobes of the gland are enucleated from the capsule (see figure 3-9). Bleeding is controlled with hemostats and ligatures, sutures, or electrocoagulation. Long forceps, half-length sutures, and long needle holders are required for placing sutures.
(6) Following removal of the prostate and control of bleeding, a hemostatic catheter with an inflatable bag--Foley 24 Fr with a 30-ml bag may be placed in the fossa; the balloon is adjusted under direct vision and inflated, using sterile water in a 30-ml syringe with an adapter. A hemostatic cone of Gelfoam may be used if preferred.
(7) The bladder is closed as for suprapubic cystostomy with a Malecot catheter in place. One or two wide Penrose drains may be placed in the prevesical space of Retzius. The wound is closed in layers and dressed.
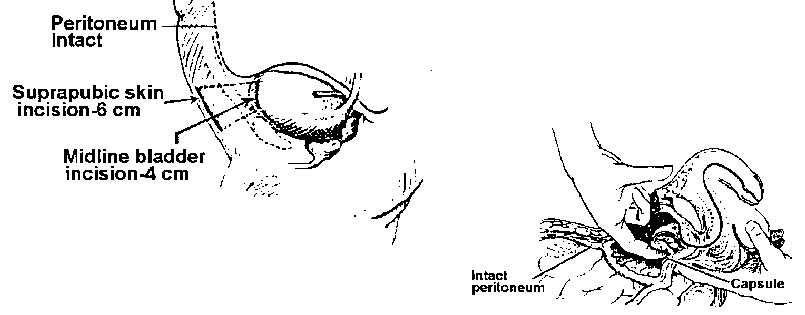
Figure 3-9. Enucleation of prostate by suprapubic approach.
