
Special Surgical Procedures II
LESSON 3: Procedures in Genitourinary Surgery
Section Iii: operations on the kidney, ureter, and adrenal glands
3-20
3-20. RECONSTRUCTIVE OPERATIONS ON THE URETER
a. General. Reconstructive operations may be indicated because of a pathological condition of the urinary bladder or lower ureter that interferes with normal drainage. Conditions requiring urinary diversion or reconstruction of the urinary tract include malignancy, cystitis, stricture, trauma, or congenital malformations such as ureteral reflux. Pelvic malignancy or an anomaly requiring removal of the bladder necessitates urinary diversion.
b. Definitions and Purposes.
(1) Ureterostomy (ureterotomy). The opening of the ureter for continued drainage from it into another part.
(2) Cutaneou-sureterostomy (anastomosis or transplant). The diversion of the flow of urine from the kidney via the ureter away from the bladder onto the skin, usually on the abdomen.
(3) Ureterectomy. The complete removal of the ureter. This procedure includes hephrectomy, as well as the excision of a cuff of the bladder.
(4) Uretero-lithotomy. An incision into the ureter and removal of a stone.
(5) Ureterou-reterostomy. The division of the ureter and reconstruction in continuity with another ureteral segment (see figure 3-7).
(6) Ureteroileostomy (ileal conduit) or ureterosigmoidostomy (anastomosis). The diversion of the ureter into a segment of the ileum or into the sigmoid colon.
(7) Ureteroneocystostomy (ureterovesical anastomosis). The division of the ureter from the urinary bladder and reimplantation of the ureter into the bladder at another site.
c. Patient Preparation. The site of incision and position of the patient will depend on the indications for surgery and the nature of the proposed reconstruction or anastomosis. The patient may be placed in a supine position for an abdominal approach or in a modified Trendelenburg position for a low abdominal or pelvic incision. The patient may also be placed in a lateral position for high ureteral stones.
d. Operative Procedure for Ureteral Anastomosis.
(1) The ureter is exposed through the desired incision. A ureteral catheter, passed retrograde, may be used to facilitate identification and isolation of the ureter. The ureter is identified and dissected free, using long forceps and scissors.
(2) The ureter is picked up with fine traction sutures, freed from the surrounding tissues, and severed at the desired level.
(3) The distal end of the ureter is ligated, and the proximal stoma is transferred to the site of anastomosis. The anastomosis is accomplished with fine dissection instruments and fine swaged-on sutures.
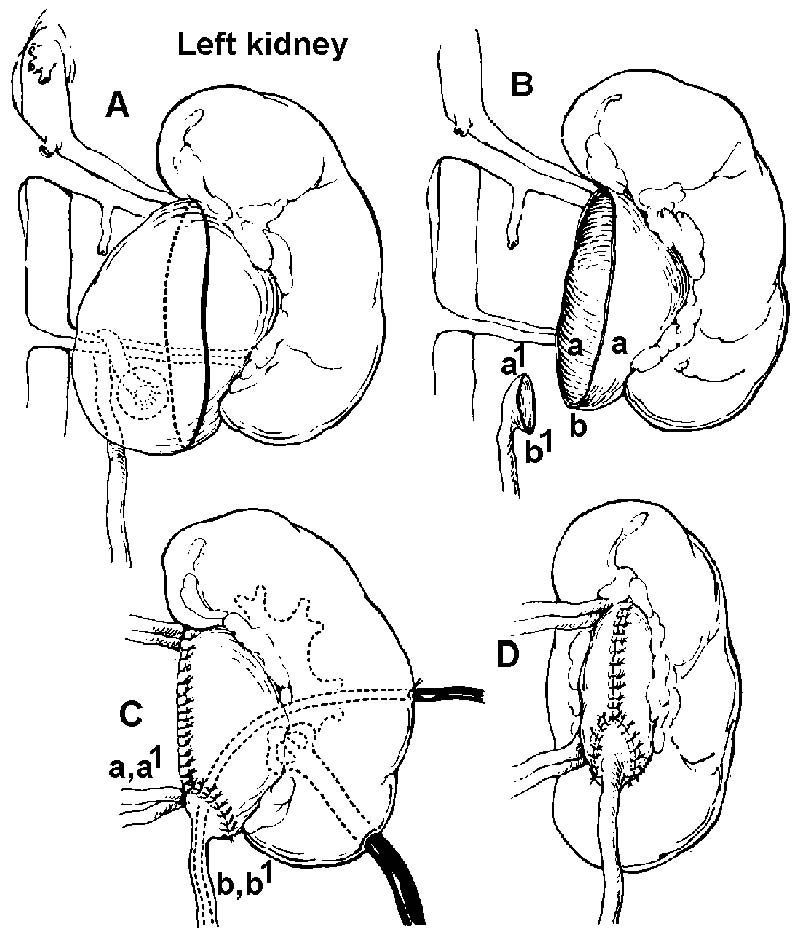
Figure 3-7. Technique of reimplantation of ureter at kidney pelvis. Correction of ureteral obstruction by aberrant vessels that cannot be divided without producing muscular renal damage.
|
A-Outline of proposed pelvic (ureteral) cuff and extent of redundant pelvic wall resection.
B-Ureter, with its funneled end, is brought approximated to dependent part of resected pelvic wall (al to aa and bl to b).
C and D-Anastomosis completed. Nephrostomy drainage and ureteral splint may be inserted. |
(4) A soft splinting catheter is usually left in place until healing has taken place and free drainage is assured.
(5) The wound is closed in layers and dressed in the routine manner.
e. Operative Procedure for Ureterolithotomy.
(1) The patient usually has a kidney, ureter, and bladder X-ray examination immediately before surgery to determine the exact location of the stone. The surgeon may also schedule a cystoscopic examination preoperatively and may attempt to manipulate the stone through the ureter.
(2) The position of the stone determines the surgical approach. A stone high in the ureter will require a flank incision, whereas one closer to the bladder will require an abdominal incision. Both of these have been described previously. The incision into the ureter is made with a small surgical blade above the stone. The Randall stone forceps will be used to locate and remove the stone. The ureter may be closed with fine chromic gut sutures number 4-0, or it may be left open and the site drained well. Either approach requires minimal routine closure.
(3) Ureterocutaneous transplant, ureterosigmoid anastomosis, and ileal segment are all urinary diversion procedures performed when the bladder no longer serves as a proper urine reservoir. The cause may be a congenital disorder (as in the neurogenic bladder), exstroptiy, trauma, or tumor.
f. Operative Procedure for Ureterocutaneous Transplant (Anastomosis). The surgical approach is the same as for a low ureterolithotomy, and the ureter is severed from the bladder. The severed ureter is passed through a stab wound in the flank and sewn to the skin with an everting suture-of number 4-0 chromic gut on an Atraumatic needle to form a stoma. The structures are handled with plastic instruments, fixation forceps, and iris scissors. A small catheter is passed into the ureter and irrigated for patency. The patient must have a urine collecting bag postoperatively.
g. Operative Procedure for Ureterosigmoid Anastomosis.
(1) The abdomen and peritoneal cavity are entered in the routine manner through a left rectus incision. A portion of the large bowel is protected with pads. Deep retractors are placed, and with long forceps and scissors the posterior peritoneum is incised.
(2) The ureters are severed close to the bladder. The ureter is brought through the posterior peritoneal incision to the sigmoid. Traction sutures and smooth tissue forceps are used to retain and handle the severed ureters.
(3) The sigmoid colon is immobilized to prevent traction and tension on the ureter by securing the former to the pelvic peritoneum at a point where the ureter falls easily on the bowel, and a silk number 3-0 traction stitch is taken. Using a scalpel with blade number 15, an incision is
made through the taenia of the sigmoid muscle layer separating it from the mucosal layer. A tunnel is created by blunt dissection.
(4) The ureter is laid on top of the mucosa, and a small-slit is made in the mucosa, using a scalpel with a number 11 blade.
(5) With fixation forceps and iris scissors, the ureter is slit to match the bowel incision. The ureter is anchored to the bowel with number 4-0 chromic ureteral sutures on Atraumatic needles. The other ureter is anastomosed in the same manner in a position slightly above the first.
(6) The posterior peritoneum is closed with fine silk sutures. Drainage is established. The abdominal wound is closed in layers.
h. Operative Procedure for Ileal Conduit.
(1) A urethral catheter is inserted to decompress the bladder, and a rectal tube is placed in the rectum. Before the incision is made, the stoma site is marked on the skin. Through a midline abdominal incision, the peritoneum is incised and the abdomen is entered in the routine manner; abdominal retractors are placed.
(2) The ureters are mobilized and brought through the retroperitoneum.
(3) The distal ileum and mesentery are inspected to identify the blood supply. A Penrose drain is passed through the mesentery midway between the two main arterial arcades adjacent to the ileum at the proximal and distal ends of the selected segment. This segment usually comprises 6 to 10 inches of the terminal ileum, a few inches from the ileocecal valve.
(4) The vessels of the mesentery are ligated. Care is exercised to preserve the ileocecal artery and adequate circulation to the isolated ileal segment. The peritoneum is incised over the proposed line of division of the mesentery. Allen or other intestinal clamps are placed across the ileum, and the bowel is divided flush with the clamps. Using gastrointestinal technique, the proximal end of the conduit is closed with a chromic layer of sutures followed by a second layer of interrupted silk sutures. The remaining ileum is reanastomosed end-to-end.
(5) The mesentery is closed with interrupted silk sutures.
(6) The closed proximal end of the conduit segment is fixed to the posterior peritoneum. The ureters are implanted in the ileal segment using plastic technique, with fine instruments and ureteral sutures of chromic number 4-0 catgut on Atraumatic needles. The peritoneum and muscle of the abdominal wall lateral to the original incision are separated by blunt dissection. The distal opening of the ileal conduit is drawn through and sewn to the skin with fine chromic or silk sutures. The wound is drained, closed, and dressed. An ileostomy bag is placed over the stoma.
NOTE: The surgeon may do a cystectomy either before or after this procedure. In
some cases, he may choose to leave the bladder rather than subject a
debilitated patient to further surgery.
