
Special Surgical Procedures II
LESSON 3: Procedures in Genitourinary Surgery
Section Iii: operations on the kidney, ureter, and adrenal glands
3-14
3-14. NEPHRECTOMY
a. General. This operation involves the removal of the kidney. It is done to treat some congenital unilateral abnormalities causing renal obstruction or severe hydronephrosis, tumor of the kidney, a severely injured kidney, renal tuberculosis, calculous pyelonephrosis, and sometimes cortical abscess.
b. Patient Preparation. The position of the patient on the operating table will depend on the type of lesion, the position of the kidney, and the surgical approach selected. The most common position for kidney operations is the lateral when a lumbar, transpleural, or extra-pleural transthoracic approach is to be used. A supine or a modified Trendelenburg position is employed when an abdominal approach is to be used.
c. Approaches to the Kidney.
(1) Lumbar or simple flank incision. This incision begins at the costovertebral angle and parallels the twelfth rib. It extends, forward and downward between the iliac crest and the thorax.
(2) Nagamatsu incision. This is a modification of the simple flank incision and is made over the eleventh and twelfth ribs, removing a section of each.
(3) Thoracoabdominal incision. The tenth and eleventh ribs are removed, and the chest cavity is opened, collapsing the lung. Rib spreaders and approximators and chest drainage are required. When the lumbar, Nagamatsu, or thoracoabdominal approach is used, the patient is placed in a lateral position.
(4) Transperitoneal and retroperitoneal incisions. The patient is placed in a supine position. A vertical incision is made in the epigastric and umbilical region on the affected side. This approach is used for a large kidney tumor or when the kidney and ureter are extensively involved in the surgery.
d. Operative Approach (Lumbar Approach).
(1) The incision is carried through the skin, fat, and fascia. Bleeding vessels are clamped with hemostats and ligated.
(2) The external oblique, the latissimus dorsi, and the internal oblique muscles are exposed. The required portions of the dorsi, external oblique, posterior inferior serratus, and internal oblique muscles are split or divided and retracted with a dull rake or Richardson right-angled retractors. Bleeding is controlled. The transversalis fascia is cut with scissors. Then the iliohypogastric and ilioinguinal nerves are identified and retracted. The sacrospinal muscle is retracted. The deep lumbar fascia is separated. The quadratus lumborum muscle may be divided.
(3) The pleura, peritoneum, and twelfth thoracic artery and nerve are identified and retracted. Laparotomy pads and Deaver retractors are placed to protect the adjacent structure and afford exposure.
(4) If necessary, a rib or ribs (twelfth, eleventh, or tenth) may be resected to give access to the kidney. The periosteum is stripped with an Alexander costal periosteotome and Doyen rib raspatory.
(5) A scalpel and heavy scissors may be used to cut through the lumbocostal ligaments. The rib is grasped with an ochsner clamp and cut with rib shears, removing the portion necessary to expose the kidney.
(6) Retractors and pads are placed. Gerota's fascia, the perirenal capsule, is grasped with long tissue forceps and incised with a scalpel. The incision is extended, using dissecting scissors, and the kidney and perirenal fat are exposed. The kidney is dissected free, using sharp and blunt dissection with long tissue forceps, scissors, and sponges on forceps. Crile hemostats are used on bleeding vessels.
(7) The ureter is identified, separated from its adjacent structures, and retracted. Holding forceps such as long Babcock or long Allis clamps may be used, or a length of Penrose tubing may be passed around the ureter to retain and retract it. The ureter is occluded by double clamping and then divided and ligated (see figures 3-6 A and B).
(8) The kidney pedicle containing the major blood vessels is isolated and doubly clamped by using long kidney clamps of a size suitable to the structures. The vessels are securely ligated with heavy chromic gut and transfixed with heavy sutures on Atraumatic needles. The pedicle is severed and the kidney removed (see figures 3-6 C and D).
(9) The wound is explored for bleeding, hemostasis secured, and the cavity cleansed by irrigating, sponging, and suctioning as necessary. A drain of Penrose tubing, which may be wicked with gauze, or a drain made of heavy rubber or plastic tubing is placed if leakage of urine is likely to occur.
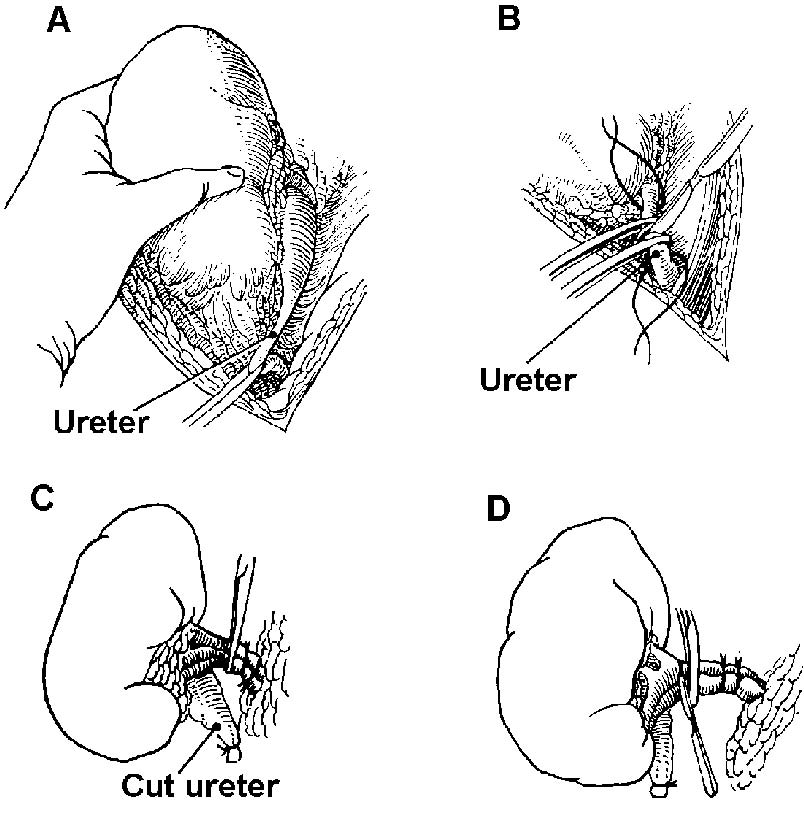
Figure 3-6. Nephrectomy.
A and B-Upper portion of ureter is freed, cut, and ligated.
C-Chromic gut ligatures are placed; kidney clamps are applied between proximal ligature and kidney itself.
D-Renal vascular pedicle is doubly ligated with suture ligatures, and the kidney is removed.
(10) The fascia and muscles are closed in layers with interrupted chromic sutures. If necessary, retension sutures may be used. The skin edges are approximated with interrupted sutures of silk or wire or with skin clips.
(11) The drain is secured and the wound dressed with gauze sponges, abdominal pads, and adhesive strips.
