
Special Surgical Procedures II
LESSON 2: Procedures in Gynecological and Obstetrical Surgery
Section Ii:
2-29
2-29. CULDOSCOPY
a. General. The diagnostic procedure provides visualization of pelvic structures through a tubular instrument similar to a cystoscope, which is introduced through a small incision in the posterior vaginal cul-de-sac. Direct observation of the passage of dye from the uterus through the fimbriated ends of the tube is possible with the culdoscope to help determine tubal patency, the presence of ectopic pregnancy, unexplained abdominal or pelvic pain, the nature of pelvic masses, and to evaluate normal functioning of the genital tract. This examination may enable the surgeon to avoid unnecessary pelvic surgery. Laparoscopy is the preferred procedure today.
b. Patient Preparation. The patient is prepared as for a vaginal operation (refer to paragraphs 2-12 and 2-13). A local or regional anesthetic may be used. When a general anesthetic is used, the patient is intubated. The patient is usually placed in a knee-chest position, kneeling on the footboard with a kneestrap around the thighs, the chest supported on pillows, and the arms comfortably flexed above the head.
c. Operating Room Preparation. Instruments may be placed on a table so that the surgeon may serve himself. However, there is still need for a circulator. The lens of the scope may fog if the instrument is introduced cold, so the tip is dipped in warm water and wiped dry before being used.
d. Operative Procedure (see figure. 2-8).
(1) The trocar of the culdoscope is inserted into the fornix behind the cervix; the trocar is then introduced into the pelvis between the two uterosacral ligaments.
(2) The trocar is withdrawn from the sheath; the sterile culdoscope is inserted through the sheath. The culdoscope does not touch the vaginal mucous membrane thus reducing the possibility of infection to a minimum.
(3) The uterus, tubes, broad ligaments, uterosacral ligaments, rectal wall, sigmoid, and small intestine may be visualized through manipulation of the scope (see figure 2-8).
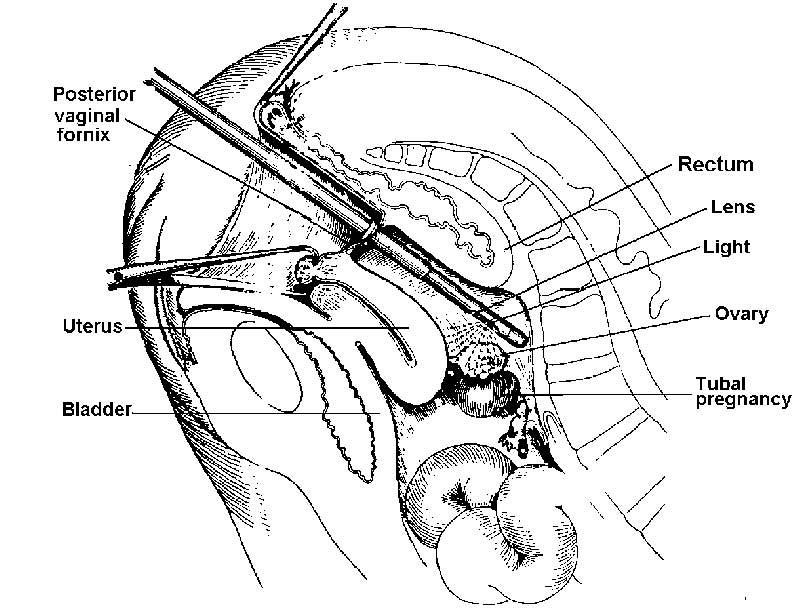
Figure 2-8. Culdoscope. Sagittal section showing culdoscopy viewing pelvic viscera.
(4) In the study of sterility, a self-retaining screw-lipped cervical cannula is introduced in the cervical canal, and it is connected by a plastic tube to a syringe containing a dye. If the uterine tube is patent, the dye solution is seen dripping from the fimbriated end.
(5) The culdoscope is withdrawn, the sheath is left in place, and the patient is placed on her side. Pressure is exerted on the abdomen to force the air out of the peritoneal cavity, thereby eliminating postoperative discomfort and potential air embolus. The vaginal wound is not sutured. The patient is returned to bed.
