 This is the Archived Desktop Edition.
This is the Archived Desktop Edition.
You should be transferred to the Newest Edition for Desktop and Mobile within 2 seconds.
Intravenous Infusions and Related Tasks
Lesson 1: Initiate an Intravenous Infusion and Manage a Patient With an Intravenous Infusion
1-3
1-3. SOLUTIONS USED IN INTRAVENOUS THERAPY
a. Resuscitation Solutions. Different types of IV fluids can be used for different medical conditions. These solutions are generally categorized as colloid or crystalloid.
(1) Colloids. Colloids contain protein, sugar, or other high molecular weight molecules and are used to expand intravascular volume. Examples include:
® (a 6 percent hetastarch solution in a balanced electrolyte solution).(a) Whole blood (most common) (see figure 1-1).
(b) Packed red blood cells (PRBC).
(c) Fresh frozen plasma (FFP).
(d) Plasma protein fraction (PPF).
(e) Hypertonic saline and dextran (HSD).
(f) Hextend
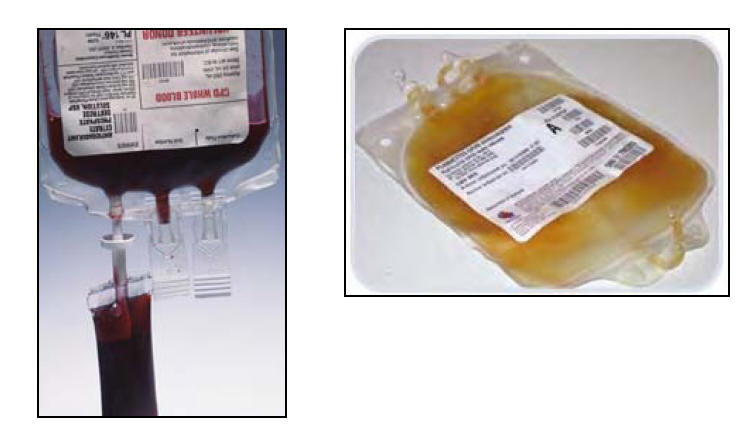
Figure 1-1. Blood products. (Left--whole blood. Right--plasma.)
(2) Crystalloids. Crystalloids are solutions that do not contain protein or other large molecules. Sodium (Na+) is the primary osmotic agent. These fluids do not remain in the vascular spaces very long. Examples include:
(a) Normal saline (NS) (0.9 percent sodium chloride [NaCl] solution).
(b) Ringer's lactate (RL).
b. Fluid Distribution. Fluids are distributed throughout the body in several different spaces and the body continually works to maintain equilibrium within these spaces. The average adult male has approximately 42 liters of fluid within the body. The fluid is distributed as follows:
(1) Intracellular space. Fluids within the cells amount to about two-thirds of the body's weight.
(2) Extracellular space. Fluids outside the cells amount to about one-third of the body's weight.
(a) Interstitial space. About eighty percent of the extracellular fluid is in spaces between tissues.
(b) Vascular space. About twenty percent of the extracellular fluid is in the circulatory system
c. Fluids.
® (about 1.3 pounds) will expand the intravascular volume by 800 ml within one hour and will sustain this expansion for up to eight hours. Hextend® contains large sugar molecules that remain in the vascular system for a much longer time than RL. Hextend® also pulls additional fluid from the interstitial spaces and holds this fluid in the vascular space for a longer period of time. Hextend® is better for treating hypovolemia secondary to blood loss than RL.(1) One thousand milliliters (ml) of Ringer's lactate (about 2.4 pounds) will expand the intravascular volume by 200 to 250 ml within one hour. Sodium is the primary osmotic agent in RL and will not remain in the vascular system very long. It diffuses out into the interstitial space and eventually into the intracellular space. This fluid is better for treating dehydration.
(2) Five hundred milliliters of Hextend
d. Resuscitation Indicators.
(1) The blood pressure is commonly used to determine who needs fluid resuscitation. However, stethoscopes and blood pressure cuffs are rarely available or useful to the front line soldier medic in the typically noisy and chaotic battlefield environment.
(2) A palpable radial pulse and normal mentation (mental ability) are adequate and tactically relevant resuscitation endpoints to either start or stop fluid resuscitation. Both can be adequately assessed in noisy and chaotic situations without mechanical devices.
(3) Casualties should only be resuscitated to a systolic blood pressure of 80 millimeters of mercury (mmHg). This blood pressure is adequate to perfuse all vital organs and, yet, not high enough to cause a possible re-bleed of a vessel that has already clotted. Re-bleeding can occur with a systolic blood pressure as low as approximately 93 mmHg.
(4) The systolic blood pressure may be approximated by palpating pulses in specific areas:
(a) A palpable carotid pulse indicates a systolic blood pressure of at least 60 mmHg.
(b) A palpable femoral pulse indicates a systolic blood pressure of at least 70 mmHg.
(c) A palpable radial pulse indicates a systolic blood pressure of at least 80 mmHg.
e. Fluid Resuscitation Algorithm.
(1) Superficial wounds. More than 50 percent of injured soldiers have only superficial wounds. These soldiers require no immediate intravenous fluids, but oral fluids should be encouraged.
(2) Significant wound. Any significant extremity (arm or leg) or truncal (neck, chest, abdomen, or pelvis) wound, with or without obvious blood loss or hypotension, may require an IV (see figure 1-2). If the casualty is coherent and has a palpable radial pulse, blood loss has likely stopped. Initiate a saline lock, hold fluids, and re-evaluate as frequently as the situation will allow. If the casualty is not nauseated, have him sip small quantities of water to assist hydration.

Figure 1-2. Significant wound to the leg.
(3) Significant blood loss. For significant blood loss from any wound where the soldier has no palpable radial pulse or is not coherent, perform the following.
®. If the mental status improves and the radial pulse returns, maintain a saline lock and hold fluids. If there is no response observed within 30 minutes, administer an additional 500 ml of(a) STOP THE BLEEDING by all means at your disposal (tourniquet, direct pressure, pressure dressing, hemostatic dressing, hemostatic powder, or other means). Many of these hypotensive casualties suffer from truncal injuries which are unaffected by these resuscitative measures (casualty may have lost as much as 1,500 ml of blood [about 30 percent of their circulating volume]).
(b) Once hemorrhage has been controlled to the extent possible, initiate IV access and administer 500 ml of Hextend
Hextend® and monitor the casualty's vital signs. If no response is seen after 1,000 ml of Hextend® has been administered, you may need to consider rationing your resources and turning your attention to more salvageable casualties.
NOTE: Remember, a liter of Hextend® is equivalent to more than six liters of Ringer's lactate.
®, the casualty is probably continuing to bleed internally. This casualty needs a rapid evacuation to a surgical facility for hemorrhage control. If you continue to give large amounts of fluids to a casualty who continues to bleed, you can speed the loss of the remaining red blood cells. This dilutes the blood’s natural ability to clot and raises the casualty's blood pressure. Doing so will actually cause the wound to bleed faster. Consequently, you only want to raise the blood pressure high enough to perfuse all the vital organs, but not enough to promote more rapid hemorrhage.(c) If a casualty’s pulse does not return after one liter of Hextend
